
Healthcare Policy
Advice or Advocacy – Varying Perceptions of Health Services and Policy Researcher Activities
P. Alison Paprica, Walter P. Wodchis and Kimberlyn M. McGrail
Abstract
The line between objective advice and advocacy may be blurred for health services and policy researchers who work closely with policy makers. Our study of 22 participants' perceptions of a five-part fictional scenario in which a researcher has increasing involvement with the ministry of health found extensive variation in what participants perceived to be objective advice or advocacy. Based on this variation, we believe that health services and policy researchers cannot completely avoid the risk of being perceived as issue advocates, whether by peers or by policy makers, and suggest some possible ways to mitigate risk.
Introduction
For more than a decade, there has been debate about the roles scientists ought to take in policy making. In his oft-cited 2007 book, Roger Pielke Jr. identifies four potential roles for scientists: the issue advocate, the honest broker of policy alternatives, the pure scientist and the science arbiter (Pielke 2007, 2015). According to Pielke's framing, pure scientists and science arbiters serve as information resources and are not concerned with specific policy decisions. In contrast, issue advocates and honest brokers both aim to inform policy making but in different ways. Honest brokers seek to expand decision alternatives, while issue advocates seek to narrow them, often to a single choice or policy option (Pielke 2007, 2015).
As noted by Goodwin (2012), there is debate in the literature regarding whether advocacy is a legitimate role for scientists, for example, some argue that scientists' special and deep knowledge imparts an obligation for them to advocate, while others view advocacy as incompatible with scientific objectivity and impartiality. Pielke contends that the four roles he identifies are each “critically important and necessary in a functioning democracy,” but that scientists must choose, i.e., “whether a scientist admits, accepts, or is aware of it, a choice must be made on how he or she relates to the decision-making process” (Pielke 2007: 7). On a related point, Oliver and Cairney's systematic review identifies “decide if you want to be an issue advocate or honest broker” as one of eight themes from the “how to influence policy” literature aimed at researchers (Oliver and Cairney 2019: 1).
Assigning the issue advocate role may be straightforward when scientists are transparent about their advocacy for broad topics such as the legitimacy of climate change, increasing the diversity of clinical trial participants and open data policies for research. However, the role that health services and policy researchers take may be less clear when their values are embedded “in the choice of question to study, the mode of study, and in the inferential gap between findings and conclusions reached” (Gluckman et al. 2021: 2). Put another way, the act of studying an intervention or policy approach because of its potential benefits or harms is unavoidably a value-laden decision regardless of whether the researchers involved in the work identify themselves as issue advocates for the object of their study. Furthermore, as Oliver and Cairney note, in order to have an impact, scientists may need to “engage with policymakers to such an extent that the division between honest broker and issue advocate become blurry” (Oliver and Cairney 2019: 6).
Notwithstanding strong incentives for academic researchers to work closely with policy makers in order to have an impact, including some research funder requirements (e.g., see Academy Health n.d.; CIHR 2023, 2024), the literature identifies potential negative consequences of the practice. Possible consequences include threats to researcher identity and autonomy (Boaz et al. 2021; Chubb and Reed 2018; Henkel 2005); insufficient yield from extensive researcher time invested in developing and maintaining relationships with policy makers (Oliver and Cairney 2019); emphasis on short-term, smaller, responsive research projects over the larger and longer-term pursuit of generalizable knowledge (McGrail et al. 2022); research evidence being used selectively and inappropriately by policy makers to add legitimacy to a policy position (Innvaer et al. 2002; Oliver and Cairney 2019); reputational damage and questions about researcher bias, independence and credibility (Oliver et al. 2019); and the politicization of research (Douglas 2015; Pielke 2007).
In practice, negative perceptions about advocacy may influence with whom peer researchers collaborate and with whom policy makers choose to work. For example, a policy maker may be hesitant to work with a researcher who previously worked on initiatives closely associated with one policy or political position. Given the potential ramifications of the roles that researchers take, we designed a study to explore whether there is consistency in the perception of specific activities of health services and policy researchers on a spectrum from objective advice to advocacy.
Twenty-two reactions to a five-part fictional scenario
We developed a five-part fictional scenario in which a researcher has increasing involvement with the ministry of health (MOH) and used it as the basis for a 45-minute real-time qualitative study at the Canadian Health Services and Policy Research Conference (CAHSPR) in May 2018 (University of Toronto Human Research Ethics Board Protocol 00035941). We began our CAHSPR session with brief oral presentations about the multiple expectations of applied health researchers, noting how this can lead to researchers being drawn into advocacy-like activities. “Advice” was defined as a “recommendation regarding a decision or course of conduct” and “advocacy” as “the act or process of supporting a cause or proposal” based on dictionary definitions (Merriam Webster n.d.). After participants provided informed consent via live electronic polling, we collected participant responses to the five parts of our scenario, which, in abbreviated form, were as follows:
- Part 1: A fictional researcher presents preliminary findings from a study of an intervention the researcher's team developed to improve the coordination of care for rural residents with multiple chronic conditions to MOH representatives, including an assistant deputy minister (ADM).
- Part 2: At the ADM's request, the researcher prepares a revised diabetes-focused version of their intervention.
- Part 3: In response to the ADM's request, the researcher provides information about the anticipated strengths and weaknesses of the diabetes-focused version of their intervention compared with an alternative US-based diabetes intervention that the MOH is considering.
- Part 4: The researcher conducts a pragmatic trial of the diabetes-focused version of their intervention with MOH funding, then joins the ADM in presenting the findings to the deputy minister and other MOH senior officials to help the ministry make an informed choice between implementing the diabetes-focused intervention at scale or a program aimed at increasing childhood vaccinations in hard-to-reach sub-populations.
- Part 5: The MOH chooses to implement the diabetes-focused version of the researcher's intervention across rural Ontario, and at the MOH's request, the researcher agrees to lead the evaluation of the implementation.
Participants used anonymous live polling to record their perceptions of the researcher's activities at each part of the five-part scenario using a 6-point Likert scale from “Completely, or almost completely, objective ADVICE” to “Completely, or almost completely, ADVOCACY” and provided open text comments with their reasons (see Table 1 noting that participants are numbered in order of increasing perception of advocacy). Participants' responses and the information provided to participants, including more detailed descriptions of each part of the scenario, are available in Appendix 1, available online here.
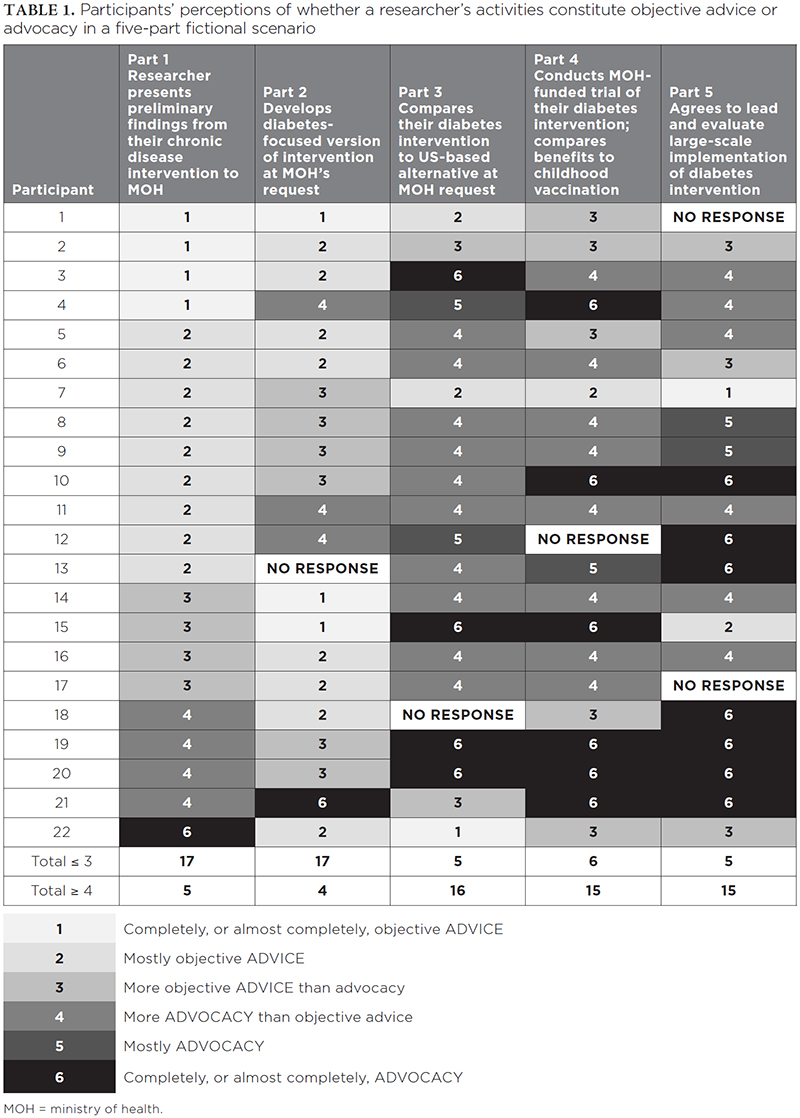
Overall, participants perceived a shift toward increased advocacy as the five-part scenario unfolded, that is, as there was greater involvement of the researcher with the MOH policy process, there was, in general, greater likelihood of perceiving advocacy. At the same time, there was variation in participants' views about what constituted objective advice or advocacy. Individual results were highly variable, with 14 of the 22 participants entering responses that did not show a consistent trend toward perceiving increasing advocacy while often identifying different parts of the scenario as having the highest perceived advocacy and for different reasons. For example, participant 3 perceived the presentation of preliminary findings to the MOH in part 1 as “Completely, or almost completely, objective ADVICE” while participant 22 perceived the same activity as “Completely, or almost completely, ADVOCACY.”
Some participants emphasized that the MOH, not the researcher, was not acting objectively. For instance, for part 2, participant 8 commented, “This feels like ministry advocacy not researcher advocacy.” Most participants seemed to draw the line between objective advice and advocacy based on whether there was potential for conflict of interest for the researcher, particularly in part 3 of the fictional scenario where the fictional researcher compares their own intervention to another intervention being considered by the MOH. Participant 16 expressed this sentiment as “Researcher is naturally inclined to work in self-interest because of funding. Scenario also speaks to need for ministry knowledge users to know how to handle these relations with researchers.”
This study has some limitations. There were a small number of participants, and even if more people had participated, the results from a convenience sample of policy conference attendees may differ from those if other participants were engaged (e.g., researchers and policy makers who did not attend the conference). Furthermore, some consented participants had technical difficulties that prevented them from responding to all questions, and we could not collect reliable data about participants' roles (i.e., researcher, trainee, patient, policy maker or decision maker). Even so, we do think the study findings have important implications.
Mitigating risks
Foremost, the study findings show that common health services and policy researcher activities, such as sharing preliminary results with policy makers, may be perceived as advocacy. In the context of guidance that recommends health researchers work with policy makers and decision makers to achieve impact (Cairney and Oliver 2017; CIHR 2015; Evans and Cvitanovic 2018; Oliver et al. 2022) and research funding competitions that require deep involvement of knowledge users in research (e.g., see Academy Health n.d.; CIHR 2023, 2024), it would be very hard for any health services and policy researcher to completely avoid advocacy-like activities. Accordingly, researchers and policy makers may want to mitigate risks.
In our view, mitigation starts with awareness. Consistent with Cairney and Oliver's guidance, health services and policy researchers need to “recognize that their decisions about how far they will go to influence policy are value-driven and political, not just ‘evidence-based’, choices” (Cairney and Oliver 2017: 1) and be transparent about the fact that they are not disinterested parties when it comes to the policy options and interventions that they develop or co-develop (Oliver et al. 2019). Transparency could be aided by researcher positionality statements, both at the start of presentations to policy makers and in publications (Jafar 2018). Fulsome positionality statements that describe a researcher's relationship to their chosen research topics – for example, if they have advocated for specific policies or have focused their careers on specific approaches – could help peer researchers and policy makers understand the nature of the space that a researcher usually operates within, and potential limits to the researcher's objectivity, thus decreasing the likelihood that a researcher will be negatively perceived as what Pielke terms a “stealth issue advocate” (Pielke 2015).
However, while positionality statements may serve to identify potential researcher conflicts of interests, they do not mitigate the real risk of conflict of interest where it exists, such as when a researcher is asked to advise about an intervention or policy that they have a strong interest in (e.g., see parts 3, 4, and 5 of the fictional scenario). In such cases, we suggest that risks could be mitigated by involving people who do not have personal stakes in the decisions under consideration, for example, by having independent scientific advisors or a steering committee provide impartial strategic advice and recommendations. Notably, this would be aligned with Pielke's recommendation that science arbitration and honest brokering of policy alternatives are best done by committee, ideally, by legitimate, authoritative bodies that are well-connected to policy makers (Pielke 2015).
Conclusions
Multiple factors naturally lead health services and policy researchers to undertake activities that are likely to be perceived as advocacy, at least by some people. The findings from our study can help health services and policy researchers and policy makers understand that some common activities in health services and policy research may be perceived as advocacy and reflect on where their own activities fall in the spectrum of advice to advocacy. Researchers should be aware that they may be perceived as issue advocates, even when their aim is to provide objective advice. Awareness, combined with transparency, for example, through researcher positionality statements, and good research governance practices, may help mitigate negative risks when researchers work closely with policy makers.
Grants
Open access publication fees were paid by the Health System Performance Network, which receives funding from the Ontario Ministry of Health (Grant No. 694) and the Ontario SPOR SUPPORT Unit.
Correspondence may be directed to P. Alison Paprica by e-mail at alison.paprica@utoronto.ca.
Conseils ou défense des intérêts – Perceptions variables de l'activité des chercheurs du domaine des services et des politiques de santé
Résumé
La frontière entre conseils objectifs et défense des intérêts peut être floue pour les chercheurs du domaine des services et des politiques de santé qui travaillent en étroite collaboration avec les décideurs. Notre étude, qui porte sur la perception de 22 participants à l'égard d'un scénario fictif en cinq volets dans lequel un chercheur s'implique de plus en plus dans le ministère de la Santé, a révélé une grande variation dans ce que les participants considèrent comme des conseils objectifs ou des activités de défense d'intérêts. Compte tenu de cette variation, nous croyons que les services de santé et les chercheurs ne peuvent pas éviter complètement le risque d'être perçus comme des défenseurs d'intérêts, que ce soit par leurs pairs ou par les décideurs, et nous suggérons certaines façons d'atténuer ces risques.
About the Author(s)
P. Alison Paprica, Phd, Senior Fellow and Professor (Adjunct), Institute for Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Senior Fellow, Massey College
Walter P. Wodchis, Phd, Professor, Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Senior Scientist and Research Chair, Implementation and Evaluation Science, Institute for Better Health, Trillium Health Partners, Mississauga, Ontario
Kimberlyn M. Mcgrail, Phd, Professor, Centre for Health Services and Policy Research, School of Population and Public Health, University of British Columbia, Vancouver, British Columbia
Acknowledgment
We thank Anita Kothari for her recommendations on relevant articles to include in the literature review.
References
Academy Health. n.d. Delivery System Science Fellowship. Retrieved June 12, 2024. <https://academyhealth.org/dssf>.
Boaz, A., R. Borst, M. Kok and A. O'Shea. 2021. How Far Does an Emphasis on Stakeholder Engagement and Co-Production in Research Present a Threat to Academic Identity and Autonomy? A Prospective Study Across Five European Countries. Research Evaluation 30(3): 361–69. doi:10.1093/reseval/rvab013.
Cairney, P. and K. Oliver. 2017. Evidence-Based Policymaking Is Not Like Evidence-Based Medicine, So How Far Should You Go to Bridge the Divide Between Evidence and Policy? Health Research Policy and Systems 15(1): 35. doi:10.1186/s12961-017-0192-x.
Canadian Institutes of Health Research (CIHR). 2015. Knowledge Translation in Health Care: Moving From Evidence to Practice. Retrieved May 31, 2024. <https://cihr-irsc.gc.ca/e/40618.html#toc>.
Canadian Institutes of Health Research (CIHR). 2023. Transforming Health With Integrated Care. Retrieved May 31, 2024. <https://cihr-irsc.gc.ca/e/52996.html>.
Canadian Institutes of Health Research (CIHR). 2024. The Health System Impact Program. Retrieved May 31, 2024. <https://cihr-irsc.gc.ca/e/51211.html>.
Chubb, J. and M.S. Reed. 2018. The Politics of Research Impact: Academic Perceptions of the Implications for Research Funding, Motivation and Quality. British Politics 13: 295–311. doi:10.1057/s41293-018-0077-9.
Douglas, H. 2015. Politics and Science: Untangling Values, Ideologies, and Reasons. The Annals of the American Academy of Political and Social Science 658(1): 296–306. doi:10.1177/0002716214557237.
Evans, M.C. and C. Cvitanovic. 2018. An Introduction to Achieving Policy Impact for Early Career Researchers. Palgrave Communications 4: 88. doi:10.1057/s41599-018-0144-2
Gluckman, P.D., A. Bardsley and M. Kaiser. 2021. Brokerage at the Science-Policy Interface: From Conceptual Framework to Practical Guidance. Humanities and Social Sciences Communications 8(1): 84. doi:10.1057/s41599-021-00756-3.
Goodwin, J. 2012. What Is “Responsible Advocacy” in Science? Good Advice. Proceedings of a Conference at Iowa State University Summer Symposium on Science Communication (pp. 151–61). Great Plains Society for the Study of Argumentation. Retrieved May 31, 2024. <https://dr.lib.iastate.edu/handle/20.500.12876/84401>.
Henkel, M. 2005. Academic Identity and Autonomy in a Changing Policy Environment. Higher Education 49: 155–76. doi:10.1007/s10734-004-2919-1.
Innvaer, S., G. Vist, M. Trommald and A. Oxman. 2002. Health Policy-Makers' Perceptions of Their Use of Evidence: A Systematic Review. Journal of Health Services Research and Policy 7(4): 239–44. doi:10.1258/135581902320432778.
Jafar, A.J.N. 2018. What Is Positionality and Should It Be Expressed in Quantitative Studies? Emergency Medicine Journal 35(5): 323–24. doi:10.1136/emermed-2017-207158.
McGrail, K., F. Clement and M. Law. 2022. The Value of and Need for Health Services and Policy Research that Focuses on Macro System-Level Challenges. Healthcare Papers 20(3): 26–32. doi:10.12927/hcpap.2022.26846.
Merriam Webster, n.d. Dictionary. Merriam Webster. Retrieved November 16, 2024. <https://www.merriam-webster.com/>.
Oliver, K. and P. Cairney. 2019. The Dos and Don'ts of Influencing Policy: A Systematic Review of Advice to Academics. Palgrave Communications 5(1): 1–11. doi:10.1057/s41599-019-0232-y.
Oliver, K., A. Hopkins, A. Boaz, S. Guillot-Wright and P. Cairney. 2022. What Works to Promote Research-Policy Engagement? Evidence and Policy 18(4): 691–713. doi:10.1332/174426421x16420918447616.
Oliver, K., A. Kothari and N. Mays. 2019. The Dark Side of Coproduction: Do the Costs Outweigh the Benefits for Health Research? Health Research Policy and Systems 17: 33. doi:10.1186/s12961-019-0432-3.
Pielke, R. 2007. The Honest Broker: Making Sense of Science in Policy and Politics. Cambridge University Press.
Pielke, R. 2015, January 19. Five Modes of Science Engagement. Roger Pielke Jr.'s Blog. Retrieved May 31, 2024. <https://rogerpielkejr.blogspot.com/2015/01/five-modes-of-science-engagement.html>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed